
 MRI Cardiac Morph & Function w wo Contrast, Other cardiomyopathies
MRI Cardiac Morph & Function w wo Contrast, Other cardiomyopathies
CARDIAC MR WITH AND WITHOUT IV CONTRAST
HISTORY: Other cardiomyopathies
COMPARISON: CT chest 1/5/2023TECHNIQUE:
TECHNIQUE: Multiplanar images of the heart were obtained at 1.5 Tesla. Morphologic and dynamic cine imaging was performed in multiple projections. 16 ml of intravenous Gadavist was administered for delayed enhancement imaging. Flow quantification sequences were obtained. Post processing included flow and volume calculations, which were performed by the interpreting physicians on an independent workstation.
FINDINGS:
Thoracic Aorta: The thoracic aorta is normal in caliber. No aneurysm or dissection is seen. The ascending aorta measures 3.8 cm in diameter.
Pulmonary artery: The main pulmonary artery is dilated, measuring 3.7 cm in diameter.
Systemic and pulmonary venous return: Conventional.
lnteratrial septum: Intact.
Cardiac chambers: Normal atrioventricular and ventriculo-arterial concordance.
Coronary arteries: Normal origins.
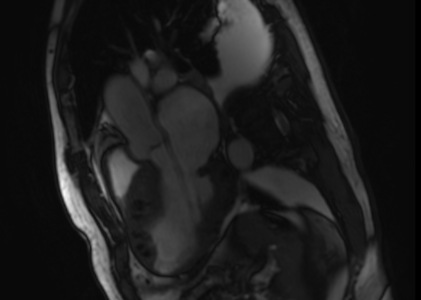
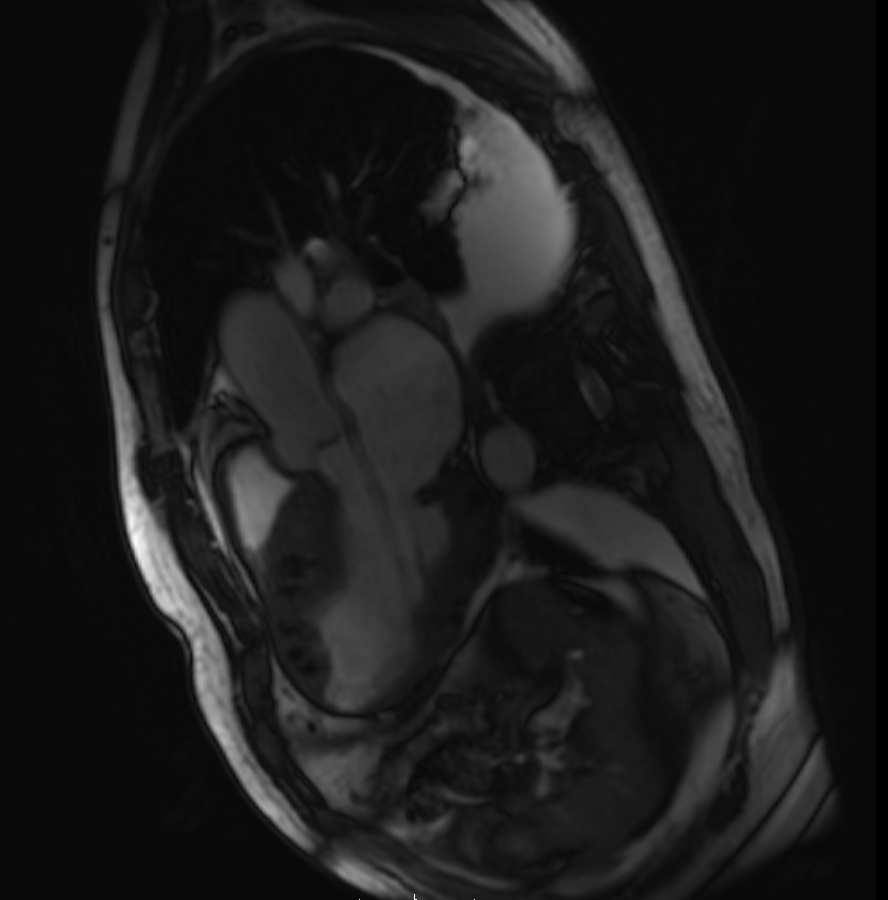
Left ventricle: The left ventricular size is moderately enlarged. Left ventricular systolic function is mildly depressed. The walls of the left ventricle are diffusely hypoknetic, with akinesia of the lateral basal wall.. There is irregular diffuse asymmetric left ventricular hypertrophy: The LV mass is severely increased. T2-weighted imaging demonstrates no high signal intensity to suggest the presence of myocardial edema. As noted on prior CT scan, there are widespread coarse calcifications throughout the myocardium. Postcontrast images demonstrate patchy delayed myocardial enhancement throughout the left ventricle. No thrombus is visible in the left ventricle. There is no systolic anterior motion of the mitral valve or outflow tract obstruction.
LV MEASUREMENTS:
BSA: 1.86 sq. m., weight 168 lb, height 66 i
LVEDV: 247 ml. LVEDVI: 133 ml/sq.m. (Normal < 95; mildly increased: 95-115; moderately increased: 116-135;
severely increased> 135 ml/sq.m)
LVESV: 147 ml. LVESVI: 79 ml/sq.m.
LVSV: 99 ml. LVSVI: 54 ml/sq.m.
LVEF: 40% (Normal 55-78%; mildly depressed: 40-54%; moderately depressed: 30-39%; severely depressed <30%) EDD: 6.1 mm (normal 43-59 mm)
ESD: 5.0 mm (normal: 26-40 mm)
Anterior septal wall: 2.4 mm (normal<12 mm)
Posterior septal wall: 2.3 mm (normal<11 mm)
LV mass: 347 g.
LV mass index: 187 g/sq.m. (Normal < 80; mildly increased: 81-99; moderately increased: 100-120; severely increased> 120 g/sq.m)
Cardiac output: 7.5 Umin
Cardiac index: 4.03 L/min/sq.m.
Right ventricle: The right ventricular size is normal. Right ventricular systolic function is globally mildly depressed. No segmental wall motion abnormalities or aneurysms are seen. Post-contrast images demonstrate no delayed myocardial enhancement. No thrombus is visible in the right ventricle.
RV MEASUREMENTS: RVEDV: 192 ml.
RVEDVI: 103 ml/sq.m. (Normal: 58-114; mildly increased: 115-171; moderately increased:
172-228; severely increased> 228 ml/sq.m)
RVESV: 110 ml. RVESVI: 59 ml/sq.m.
RVSV: 83 ml. RVSVI: 45 ml/sq.m.
RVEF: 43% (Normal >46%; mildly depressed: 36-46%; moderately depressed: 25-35%; severely depressed <25%)
Left atrium: The left atrial size is moderately enlarged, measuring 5.3 cm AP in end systole (Normal: 3.1-4.3). No thrombus is visible in the left atrium.
Right atrium: The right atrial size is normal, measuring 3.6 cm AP in end systole on the four-chamber view (Normal:
3.0-4.5). No thrombus is visible in the right atrium.
Aortic valve: The aortic valve is tricuspid, with marked sclerosis of the aortic valve leaflets. There is moderate aortic stenosis, with an open valve area of 1.4 sq cm and a maximal forward velocity of less than 300 emfs. There is mild aortic regurgitation, with a 16% regurgitant fraction. Phase-contrast imaging at the ascenqing aorta reveals a forward flow of 48 cc/heart beat.
Pulmonic valve: There is no significant pulrr, bnic stenosis or regurgitation. Phase-contrast imaging at the main pulmonary artery reveals a forward flow of 52 cc/heart beat.
Qp/Qs: Normal.
Mitral valve: There is no significant mitral stenosis or regurgitation.
Tricuspid valve: There is no significant tricuspid stenosis or regurgitation.
Pericardium: No pericardia! thickening, enhancement or pericardia! effusion is identified.
Lungs and pleura: There are moderate bilateral pleural effusions, comparable to the prior CT scan. Limited evaluation of the lungs demonstrates no abnormal signal characteristics.
Visualized upper abdominal organs: Unremarkable.
IMPRESSION: Markedly abnormal appearance of the left ventricle, with extensive dystrophic myocardial calcifications associated and asymmetric and irregular diffuse myocardial hypertrophy. LV mass is severely increased. Left ventricular chamber size is enlarged, with mildly depressed systolic function. Ejection fraction equals 40%. There is patchy delayed gadolinium enhancement of the myocardium diffusely. Differential possibilities include myocarditis, sarcoidosis, amyloid
infiltration or monoclonal gammopathy.
Normal right ventricular chamber size, with mildly depressed systolic function. Ejection fraction equals 43%. Moderately enlarged left atrium. Normal size right atrium.
Moderate aortic stenosis, with extensive sclerosis of the tricuspid aortic valve leaflets. Valve opening area of 1.3 cm sq, with a maximal forward flow velocity of less than 300 emfs. Mild aortic regurgitation, with a 16% regurgitant fraction. Relatively normal appearance of the pulmonic, mitral and tricuspid valves.
Moderate bilateral pleural effusions. No pericardia! effusion.
Normal caliber ascending aorta.
Dilated main pulmonary artery, suggestive of pulmonary arterial hypertension.