
Myocarditis and Pericarditis — How Cardiac MRI Helps Diagnose Heart Inflammation
Table of Contents
- 1 Myocarditis and Pericarditis — How Cardiac MRI Helps Diagnose Heart Inflammation
- 2 What Are Myocarditis and Pericarditis?
- 3 Why Cardiac MRI Is the Gold Standard for Evaluating Heart Inflammation
- 4 How Cardiac MRI Evaluates Myocarditis
- 5 How Cardiac MRI Evaluates Pericarditis
- 6 What to Expect During a Cardiac MRI for Myocarditis or Pericarditis
- 7 Frequently Asked Questions
What Are Myocarditis and Pericarditis?
Myocarditis
Myocarditis is inflammation of the myocardium — the heart’s muscular wall. It is most often triggered by viral infections, including influenza, Coxsackievirus, and, more recently, SARS-CoV-2 (COVID-19). Other causes include autoimmune diseases, certain medications, and toxic exposures. In many cases, the cause remains unknown (idiopathic).

Symptoms vary widely. Some patients experience only mild chest discomfort and fatigue. Others develop more serious symptoms, including shortness of breath, palpitations, and abnormal heart rhythms (arrhythmias). In rare but severe cases, myocarditis can lead to acute heart failure or sudden cardiac arrest, particularly in younger, otherwise healthy individuals.
Pericarditis
Pericarditis is inflammation of the pericardium, the thin fibrous sac surrounding and protecting the heart. Like myocarditis, it is most commonly caused by viral infection, but it can also result from bacterial infection, autoimmune disorders (such as lupus or rheumatoid arthritis), kidney failure, or as a complication after cardiac surgery or a heart attack.
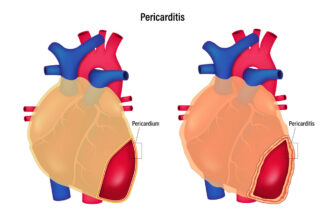
The hallmark symptom is sharp chest pain that often improves when the patient sits up and leans forward. A pericardial friction rub, a scratching sound heard through a stethoscope, and fever are also common. Pericarditis can present as an acute episode, a recurrent condition, or, in chronic cases, as constrictive pericarditis, in which a thickened, scarred pericardium restricts normal heart function.
When Both Conditions Overlap: Myopericarditis
In some patients, inflammation affects both the myocardium and the pericardium — a condition called myopericarditis. Determining which structure is primarily involved and to what extent has direct implications for treatment and prognosis. Cardiac MRI is uniquely capable of mapping involvement of both structures in a single examination.
Why Cardiac MRI Is the Gold Standard for Evaluating Heart Inflammation
Before cardiac MRI became widely available, diagnosing myocarditis often required an endomyocardial biopsy — an invasive procedure with its own risks and a recognized sampling error problem because inflammation is not always uniformly distributed throughout the heart muscle. Cardiac MRI changed that.
CMR offers several distinct advantages for evaluating inflammatory heart disease:
It provides superior soft-tissue characterization compared with echocardiography or CT, allowing direct visualization of edema, active inflammation, and scarring within the heart muscle and pericardium.
It can distinguish myocarditis from an acute myocardial infarction (heart attack) — a critical clinical distinction, since both conditions can present with chest pain and elevated cardiac biomarkers.
It evaluates the heart’s structure, function, and tissue characteristics in a single exam.
It involves no ionizing radiation.
It can be repeated over time to monitor disease progression or treatment response without incurring cumulative radiation risk.
How Cardiac MRI Evaluates Myocarditis
Several complementary MRI sequences are used together to build a complete picture of myocardial inflammation:
T2-Weighted Imaging detects myocardial edema — excess fluid within the heart muscle that is a direct marker of active inflammation. Regions of edema appear bright on T2-weighted images, helping localize and quantify the extent of acute injury.
Early Gadolinium Enhancement (EGE) is performed shortly after the injection of a gadolinium-based contrast agent. Abnormal early enhancement indicates increased vascularity and capillary leak — features consistent with active inflammatory injury.
Late Gadolinium Enhancement (LGE) is the most diagnostically powerful sequence. Performed approximately 10 minutes after contrast injection, LGE reveals areas of myocardial necrosis and fibrosis (scar tissue). In myocarditis, the LGE pattern is characteristically non-ischemic: enhancement typically appears in the epicardial (outer) layer or mid-wall of the myocardium and tends to spare the subendocardium (inner layer). This pattern contrasts with the subendocardial or transmural enhancement seen after a true heart attack, allowing the two conditions to be reliably differentiated.
T1 and T2 Mapping are quantitative techniques that assign numerical values to tissue characteristics across the heart muscle. Mapping provides a more objective, reproducible assessment than visual inspection alone and can detect subtle or diffuse inflammation that may not be apparent on standard sequences.
Together, these sequences form the basis of the Lake Louise Criteria, the internationally accepted CMR diagnostic framework for myocarditis, updated in 2018 to incorporate newer mapping techniques. A positive Lake Louise CMR result, in the appropriate clinical context, supports a diagnosis of myocarditis and may allow treatment decisions to be made without the need for biopsy.
How Cardiac MRI Evaluates Pericarditis
Cardiac MRI is equally valuable for assessing pericardial inflammation and its consequences:
Pericardial enhancement on LGE is the most direct indicator of active pericardial inflammation. An inflamed pericardium takes up gadolinium contrast and appears bright on delayed enhancement images, a finding that directly correlates with the degree of active disease.
Pericardial thickening can be precisely measured on MRI, helping determine whether the disease has progressed from an acute or fibrinous stage to a more chronic, constrictive form.
Pericardial effusion, fluid accumulation around the heart, is clearly visualized on MRI, including its distribution, volume, and characteristics, which can help distinguish simple inflammatory effusion from more complex or hemorrhagic collections.
T2 imaging and edema assessment help differentiate active inflammation from inactive scar or fibrosis, which is especially important in patients with recurrent pericarditis who are being considered for anti-inflammatory therapy.
Constrictive pericarditis. where a rigid, scarred pericardium restricts normal heart filling, can be assessed with cine MRI sequences that demonstrate the characteristic septal bounce (an abnormal septal motion caused by ventricular interdependence) and identify pericardial calcification or adhesions. This distinction from restrictive cardiomyopathy is clinically important because constrictive pericarditis may be surgically correctable.
What to Expect During a Cardiac MRI for Myocarditis or Pericarditis
Cardiac MRI is a non-invasive exam performed in a strong magnetic field. Most exams for myocarditis or pericarditis use gadolinium-based contrast, injected intravenously during the scan to enable the enhancement sequences described above. In patients with impaired kidney function, contrast use is evaluated on a case-by-case basis.
Because the heart is a moving structure, the scanner uses ECG gating to synchronize image acquisition with your heartbeat. You will be asked to hold your breath for short intervals during certain sequences to minimize motion artifact. Most cardiac MRI exams take 45 to 75 minutes.
For detailed preparation instructions — including what to eat and drink, medications, and what to wear — please visit GWIC’s MRI preparation page. [Internal link to patient prep page]
Frequently Asked Questions
Yes. CMR is the preferred noninvasive tool for evaluating post-viral and post-COVID myocarditis. Studies after COVID-19 have shown myocardial edema, inflammation, and LGE in some patients, including those with mild or asymptomatic initial illness. Cardiac MRI can identify these findings and help guide management.
The pattern of late gadolinium enhancement is the key differentiator. A heart attack causes scarring in a subendocardial or transmural distribution — the pattern follows the territory of the affected coronary artery. Myocarditis causes epicardial or mid-wall enhancement that does not follow coronary artery territories. This distinction is among the most clinically valuable applications of cardiac MRI.
Not in most cases. When cardiac MRI findings are consistent with myocarditis, and the clinical picture aligns, the diagnosis can generally be made without biopsy. Biopsy may still be considered when the diagnosis remains uncertain, when giant cell myocarditis or other specific pathologies are suspected, or when treatment decisions depend on histological confirmation.
MRI is safe in most patients with arrhythmias, but arrhythmias can affect image quality because the scanner relies on a regular heartbeat for ECG gating. The GWIC team will review your cardiac history before the exam and adjust protocols as needed to optimize image quality and your comfort.
Cardiac MRI images are interpreted by a radiologist with expertise in cardiac imaging. Results are typically communicated to your referring physician within one to two business days. Your physician will then discuss the findings and next steps with you.
GWIC offers MR imaging services, including an MRI brain scan that helps to diagnose and monitor many neurological conditions. Contact GWIC for all your MR imaging needs.
References
Ferreira VM, Schulz-Menger J, Holmvang G, et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. Journal of the American College of Cardiology. 2018;72(24):3158–3176. https://www.jacc.org/doi/10.1016/j.jacc.2018.09.072
RadiologyInfo.org — Cardiac MRI. Radiological Society of North America. https://www.radiologyinfo.org/en/info/cardiacmr
Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. European Heart Journal. 2015;36(42):2921–2964. https://academic.oup.com/eurheartj/article/36/42/2921/2293375